
Living with the complexities of obesity management in a busy clinic can be extremely difficult and frustrating. You may feel like you are doing everything right to help your patients access essential medications, only to find them stuck in a retail pharmacy bottleneck for weeks. Did you know that a major structural shift is now occurring in how these metabolic therapies reach the patient? The Direct-to-Consumer GLP-1 Model, pioneered by platforms such as LillyDirect, is changing the field of obesity medicine. It bypasses traditional retail paths and integrates telehealth directly into the supply chain. While it offers a pathway to access Zepbound, it also raises questions about continuity of care and the role of the primary physician. In this blog post, we will discuss how this model works, the clinical data behind DTC telemedicine, and what it means for your practice.
What is the Direct-to-Consumer GLP-1 Model?
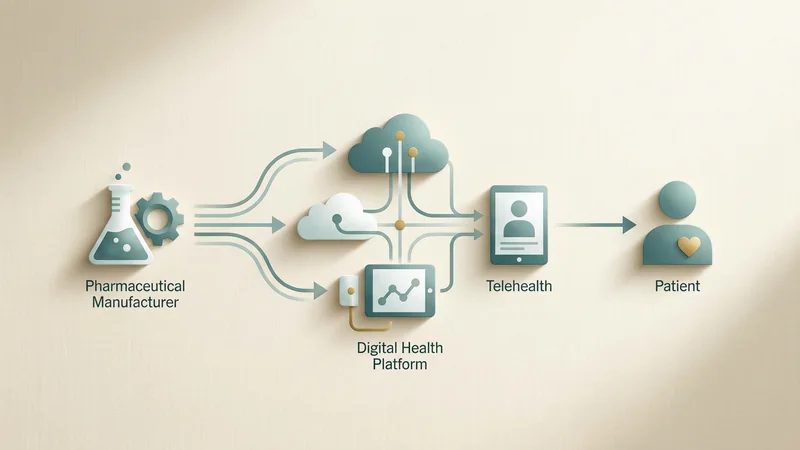
The Direct-to-Consumer GLP-1 Model is essentially a pharmaceutical-led strategy to link drug production directly with patient delivery. In the past, a patient would visit a physician, receive a prescription, and then hope their local pharmacy had the medication in stock. However, LillyDirect has changed this by offering a direct pathway for patients to access Zepbound. By integrating telehealth consultations into their own supply chain, they have created a streamlined process that moves the patient from diagnosis to delivery within a single ecosystem. This represents a major structural shift in how pharmaceutical companies distribute high-demand metabolic therapies directly to consumers.
Innovation in digital health technology to promote weight control is not a new concept (Thomas et al, *Current diabetes reports* 2014). For over a decade, researchers have looked at how digital tools can help patients stay on track with their weight loss goals. What makes the current model different is the scale and the direct involvement of the drug manufacturer. The platform allows patients to initiate care without ever stepping foot into a traditional clinic. This can be very appealing to patients who feel stigmatized in medical settings or those who live in areas with few metabolic specialists.
The shift from retail to direct delivery
Besides this, the shift removes the uncertainty of the retail pharmacy experience. Many patients on GLP-1 therapy have faced inconsistent stock levels and high out-of-pocket costs at the counter. The Direct-to-Consumer GLP-1 Model aims to stabilize this by shipping the medication directly from a centralized distributor. This ensures that the patient receives the drug they were prescribed without the common “out of stock” notification from a local pharmacist. Undoubtedly, this improves the patient experience, but it also means the patient may bypass the clinical oversight that a traditional pharmacy provides.
Bypassing traditional retail pharmacy bottlenecks
One of the primary drivers behind this new model is the ongoing frustration with retail pharmacy supply chains. Patient access to GLP-1 receptor agonists has often been limited by stock shortages and administrative delays at the local level. Retail pharmacies are often overwhelmed by the volume of prescriptions for these drugs. In some cases, pharmacists have to spend hours verifying insurance coverage or searching for available pens in nearby stores. The DTC model seeks to solve these bottlenecks by controlling the distribution from the manufacturer to the patient’s doorstep.
However, the traditional model often leaves metabolic specialists out of the loop once the prescription is sent. When a patient uses a direct platform, the local physician may not know if the medication was actually delivered or if the patient started the treatment. This can create a gap in the clinical record. Moreover, the lack of a face-to-face interaction at the pharmacy counter means there is one less professional checking for potential drug interactions or providing injection training. While the direct model is efficient, it does move the care further away from the community setting.
Impact on patient retention in traditional clinics
For a metabolic specialist, this shift can also affect patient retention strategies. If a patient finds it easier to get their medication and follow-up through a manufacturer-backed platform, they may see less of a reason to return to your clinic for regular visits. This is particularly true if the platform offers lower prices or more convenient shipping. You must handle these changes by emphasizing the value of the all-rounded care you provide. Your clinic offers more than just a prescription; it offers a long-term partnership in metabolic health that a digital platform may struggle to replicate.
Telehealth integration and the patient experience
The way LillyDirect integrates telehealth into the supply chain is a significant part of the Direct-to-Consumer GLP-1 Model. By offering built-in consultations, the platform can capture patients at the point of interest. A person who sees an ad for Zepbound can click a link and be talking to a provider within minutes. This speed is unmatched by most traditional clinics. However, the depth of these consultations can vary. Research has shown that the visit experience and fulfillment of care needs in primary care can differ significantly for video visits compared to in-person and chat visits (Söderberg et al, *Journal of general internal medicine* 2024).
In the Söderberg study, patients reported different levels of satisfaction depending on the medium used. While video visits are often efficient, some patients feel they do not get the same level of attention as they do in person. In that case, you might wonder if the subtle clinical signs of metabolic distress are being missed. For example, a video visit cannot replace a physical exam for checking injection site reactions or monitoring for muscle wasting. These are essential parts of managing a patient on high-dose GLP-1 therapy.
Balancing convenience with clinical depth
What’s more, the patient-provider relationship in a DTC setting is often transactional. The provider may be an independent contractor who does not have access to the patient’s full medical history. This is a far cry from the continuous care provided by a primary care physician or a metabolic specialist. While the platform may offer some all-rounded results in terms of weight loss, the lack of continuity can lead to fragmented care. If the patient experiences a side effect, they may not know whether to contact the platform’s provider or their local doctor.
Clinical characteristics of DTC telemedicine patients
When we look at who is using these direct platforms, the data is quite revealing. An observational cross-sectional study of 20,000 patients using direct-to-consumer telehealth found specific weight loss practices and characteristics in this cohort (Horn et al, *JMIR formative research* 2023). Most of these patients were younger and more tech-savvy than the average obesity patient seen in a traditional clinic. They were also more likely to be seeking a specific brand-name medication. This suggests that the Direct-to-Consumer GLP-1 Model is attracting a particular demographic that values speed and brand access over traditional clinical relationships.
Moreover, a 2025 study on GLP-1 receptor agonist therapy via DTC telemedicine showed that patient characteristics and treatment outcomes are comparable to traditional settings in some metrics (Gratzke et al, *Digital health* 2025). The study found that patients were able to achieve significant weight loss through these platforms. However, there are still nuances that need to be addressed. Managing these patients requires more than just a prescription. It requires an understanding of how the medication interacts with their unique physiology.
Appetite suppression and metabolic signatures
For instance, the mechanism of appetite suppression involves an inter-organ neural circuit that is highly complex (Zhang T et al, *Cell* 2022). Every patient responds differently to GLP-1 stimulation based on their neural and metabolic variability. Some clinicians are now using artificial intelligence platforms to better understand these variability signatures (Landau J et al, *Biomedicines* 2025). This level of metabolic profiling is essential to enhance treatment responses. It is unclear if a standard DTC platform has the capability or the clinical time to delve into these metabolic signatures for every patient.
The risk of missing underlying pathology
While convenience is a major selling point of the Direct-to-Consumer GLP-1 Model, there are real clinical risks to consider. Some research suggests that internet-based prescription platforms can overlook crucial pathology that would be found during a traditional office evaluation (Shahinyan RH et al, *Urology* 2020). Although the Shahinyan study focused on erectile dysfunction, the principles apply to obesity medicine as well. Obesity is rarely an isolated issue. It is often connected to other metabolic, cardiovascular, and endocrine problems that require a thorough physical exam.
Yes, the medication is effective, but it is not a silver bullet. If a patient is started on Zepbound through a platform without a proper screen for thyroid issues or gallbladder disease, the consequences could be serious. Besides this, a traditional office evaluation allows the physician to check blood pressure, heart rate, and metabolic markers in person. These are essential safety checks that ensure the patient is a good candidate for the medication. Without these checks, the platform is essentially relying on the patient’s self-reported data, which can be inaccurate.
Clinical counter-evidence and limitations
Undoubtedly, many patients will do well on these platforms, but we must look at the limitations. In the Shahinyan study, a significant portion of patients had underlying conditions that the DTC platform missed. In a metabolic setting, this could mean missing a case of pre-diabetes or an early-stage metabolic disorder. The clinician-honest view is that while AI and digital health are helpful, they are not yet a full replacement for human clinical judgment in a physical setting. A video call simply cannot provide the same diagnostic clarity as a hands-on examination.
Adherence and safety in the DTC landscape
Patient safety and adherence are always top priorities in obesity medicine. In other DTC areas, such as oral contraception, studies have evaluated patient-reported adherence and safety with mixed results (Hillen C et al, *Telemedicine journal and e-health* 2024). The Hillen study found that while patients were generally satisfied, there were gaps in their understanding of how to use the medication correctly. For GLP-1 therapies, which require careful titration to manage gastrointestinal side effects, these gaps can lead to patients stopping the medication early.
If you’re wondering how patients fare without their regular PCP, the answer often lies in the quality of the digital follow-up. A patient on Zepbound needs to know how to manage nausea, diarrhea, and other common issues. If the only support they have is a chat bot or a generic FAQ page, they may feel unsupported. Moreover, long-term adherence to these drugs is essential for maintaining weight loss. Without the accountability of an in-person visit, patients may be more likely to drift away from their treatment plan.
Pediatric considerations in digital weight management
The application of telemedicine to pediatric obesity has also provided some lessons over the past decade (DeSilva S et al, *Telemedicine journal and e-health* 2021). While the LillyDirect platform is currently for adults, the rise of digital weight management for younger populations is a growing trend. The DeSilva study highlighted the importance of involving the entire family and providing continuous support. This is something that a direct-to-consumer model for adults should also consider. Managing obesity is a behavioral and physiological challenge that requires a support system, not just a delivery service.
GLP-1 therapies and long-term health outcomes
The benefits of GLP-1 receptor agonists extend far beyond simple weight loss. Research has shown that these medications may reduce the risk of 13 obesity-associated cancers in patients with type 2 diabetes (Wang L et al, *JAMA network open* 2024). There is also evidence suggesting a lower risk of colorectal cancer in both drug-naive patients with and without obesity (Wang L et al, *JAMA oncology* 2024). These are powerful findings that highlight why access to these medications is so essential. Given the global burden of disease and the risk-attributable burden of obesity (GBD 2023 collaborators, *Lancet* 2025), getting these drugs to the right people is a public health priority.
The Direct-to-Consumer GLP-1 Model is one way to scale this access. By removing the traditional barriers of pharmacy stock and specialist availability, the model could help thousands of people reduce their long-term health risks. However, the mortality and life expectancy estimates for different countries show that obesity remains a primary driver of death (GBD 2023 Demographics Collaborators, *Lancet* 2025). To make a real dent in these numbers, we need more than just direct shipping. We need a system that ensures patients stay on their medication and receive the all-rounded care they need to manage their metabolic health.
Addressing the global burden of disease
The Lancet studies from 2025 emphasize that the global burden of 292 causes of death is still heavily influenced by metabolic risk factors (GBD 2023 Causes of Death Collaborators, *Lancet* 2025). Undoubtedly, GLP-1 therapies are a key part of the solution. But access must be paired with safety. If the Direct-to-Consumer GLP-1 Model leads to more people taking the drug but fewer people getting their blood pressure or kidney function checked, we may see new health problems arise. It is a balancing act that requires clinicians to stay engaged with their patients, even if those patients are using digital platforms.
Structural actions and receptor pharmacology
Understanding why these drugs work so well is essential for any metabolic specialist. Tirzepatide, for example, has multiplexed pharmacological actions at the GIP, GLP-1, and glucagon receptors (Zhao F et al, *Nature communications* 2022). This structural insight explains the high efficacy seen in clinical trials. The drug targets multiple pathways to improve insulin sensitivity and reduce appetite. However, the Direct-to-Consumer GLP-1 Model focuses more on the logistics of distribution than the intricacies of pharmacology.
As a clinician, you know that the drug is only part of the equation. The other part is how the patient’s body responds over time. If a patient is on tirzepatide but their GIP response is not what was expected, they may need a dose adjustment or a change in their lifestyle plan. This is where the clinical expertise of a specialist is essential. A DTC platform that uses a “one size fits all” titration schedule may not be providing the best care for every patient. Yes, the structural actions of the drug are impressive, but they must be managed within a clinical framework.
The role of metabolic variability
Every patient has a unique metabolic variability signature. Using an artificial intelligence platform to enhance treatment responses by utilizing these signatures is a promising new direction (Landau J et al, *Biomedicines* 2025). This approach recognizes that obesity is not a single disease but a spectrum of metabolic states. If the Direct-to-Consumer GLP-1 Model can eventually incorporate this kind of personalized data, it could become a more effective clinical tool. For now, it remains a distribution-focused model that requires local clinicians to fill in the gaps in personalized care.
Is the DTC model a sustainable solution?
Undoubtedly, the field of obesity medicine is changing. The direct-to-consumer pathway offers an all-rounded solution for access, but it may lead to fragmented care in the long run. If a patient gets their Zepbound through a platform like LillyDirect, their primary care provider may not have the full picture of their treatment. This can lead to issues with medication reconciliation and long-term health monitoring. However, if these platforms can better integrate with existing medical records, they could become a powerful tool in the fight against obesity.
For now, it remains a major structural shift that metabolic specialists must address to protect their patient retention strategies. You can find success by emphasizing the human element of care. Patients still value the relationship they have with their doctor, especially when it comes to a sensitive issue such as weight management. By offering the latest evidence-based care and an all-rounded approach, you can ensure your patients stay with you for the long term.
Conclusion
Undoubtedly, the Direct-to-Consumer GLP-1 Model is more than just a new way to buy medicine. It is a fundamental change in the healthcare delivery system that clinicians must understand. This model has shown that pharmaceutical companies can successfully bypass traditional retail pharmacy hurdles to reach patients directly. However, it also highlights the essential need for continuity of care and thorough clinical evaluation. As we move forward, it will be vital to see how traditional clinics and these new digital platforms can work together for the patient’s benefit. If we focus on the patient’s long-term metabolic stability, we can ensure that these powerful therapies are used safely and effectively. You can rest assured that metabolic medicine will continue to evolve, and staying informed is the best way to manage your practice in this new era.
References
- Horn DB et al. Characteristics and Weight Loss Practices From a Cohort of 20,000 Patients Using Direct-to-Consumer Telehealth: Observational Cross-sectional Study. JMIR formative research 2023. doi:10.2196/40062 (PMID: 36602855)
- Gratzke M et al. GLP-1 receptor agonist therapy for obesity via direct-to-consumer telemedicine: Clinical characteristics and treatment outcomes. Digital health 2025. doi:10.1177/20552076251382040 (PMID: 41000573)
- GBD 2023 Causes of Death Collaborators. Global burden of 292 causes of death in 204 countries and territories and 660 subnational locations, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023. Lancet (London, England) 2025. doi:10.1016/S0140-6736(25)01917-801917-8) (PMID: 41092928)
- GBD 2023 Disease and Injury and Risk Factor Collaborators. Burden of 375 diseases and injuries, risk-attributable burden of 88 risk factors, and healthy life expectancy in 204 countries and territories, including 660 subnational locations, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023. Lancet (London, England) 2025. doi:10.1016/S0140-6736(25)01637-X01637-X) (PMID: 41092926)
- DeSilva S et al. The Application of Telemedicine to Pediatric Obesity: Lessons from the Past Decade. Telemedicine journal and e-health : the official journal of the American Telemedicine Association 2021. doi:10.1089/tmj.2019.0314 (PMID: 32293986)
- Shahinyan RH et al. Direct-To-Consumer Internet Prescription Platforms Overlook Crucial Pathology Found During Traditional Office Evaluation of Young Men With Erectile Dysfunction. Urology 2020. doi:10.1016/j.urology.2020.03.067 (PMID: 32535075)
- Hillen C et al. Evaluating Patient-Reported Adherence And Safety for Oral Contraception Treatment in Women via a Direct-To-Consumer Prescription Platform: A Cross-Sectional Study. Telemedicine journal and e-health : the official journal of the American Telemedicine Association 2024. doi:10.1089/tmj.2024.0168 (PMID: 39231301)
- GBD 2023 Demographics Collaborators. Global age-sex-specific all-cause mortality and life expectancy estimates for 204 countries and territories and 660 subnational locations, 1950-2023: a demographic analysis for the Global Burden of Disease Study 2023. Lancet (London, England) 2025. doi:10.1016/S0140-6736(25)01330-301330-3) (PMID: 41092927)
- Thomas JG et al. Review of innovations in digital health technology to promote weight control. Current diabetes reports 2014. doi:10.1007/s11892-014-0485-1 (PMID: 24664797)
- Söderberg D et al. Visit Experience and Fulfillment of Care Needs in Primary Care Differs for Video Visits Compared to In-person and Chat Visits. Journal of general internal medicine 2024. doi:10.1007/s11606-024-08781-z (PMID: 38758339)
- Zhang T et al. An inter-organ neural circuit for appetite suppression. Cell 2022. doi:10.1016/j.cell.2022.05.007 (PMID: 35662413)
- Wang L et al. Glucagon-Like Peptide 1 Receptor Agonists and 13 Obesity-Associated Cancers in Patients With Type 2 Diabetes. JAMA network open 2024. doi:10.1001/jamanetworkopen.2024.21305 (PMID: 38967919)
- Landau J et al. Employing an Artificial Intelligence Platform to Enhance Treatment Responses to GLP-1 Agonists by Utilizing Metabolic Variability Signatures Based on the Constrained Disorder Principle. Biomedicines 2025. doi:10.3390/biomedicines13112645 (PMID: 41301738)
- Zhao F et al. Structural insights into multiplexed pharmacological actions of tirzepatide and peptide 20 at the GIP, GLP-1 or glucagon receptors. Nature communications 2022. doi:10.1038/s41467-022-28683-0 (PMID: 35217653)
- Wang L et al. GLP-1 Receptor Agonists and Colorectal Cancer Risk in Drug-Naive Patients With Type 2 Diabetes, With and Without Overweight/Obesity. JAMA oncology 2024. doi:10.1001/jamaoncol.2023.5573 (PMID: 38060218)
- https://www.fiercehealthcare.com/digital-health/insiders-look-lillydirect
Licensed physician and clinical AI specialist. Founder and Editor-in-Chief of ZayedMD, a physician-led medical publication covering clinical AI, neurology, metabolic health, and evidence-based patient guidance.


